
























"Jesus had compassion on them and touched their eyes: and immediately
their eyes received sight, and they followed him."
~ Matt. 20:34
Vision Outreach International began in 2001 through short-term mission endeavors. Since that time VOI has grown into a MAJOR advocate for helping the blind and the poor in under-served regions of the world.
Changing Lives !
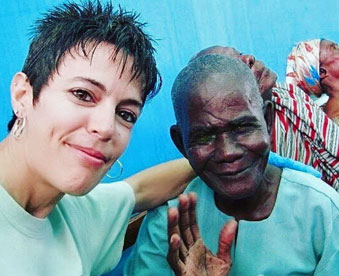
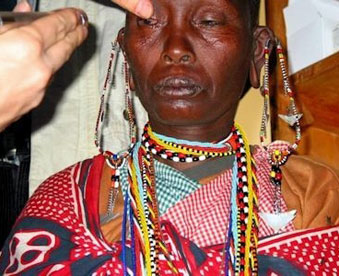
A young mother in Tanzania was trying to give her three children to a young American missionary. “I’m dying so take my children and raise them as your own.” Her husband had abandoned her, society had rejected her, and the government wouldn’t help her because the lady was blind. She came to our clinic and her sight was restored. This mother and her children were rescued from poverty and death. As a result of the love that was shown her, she also became a Christ Follower!
A young man in Ecuador tried everything to improve his vision. No matter where he went, no one would give him hope of ever seeing again. Because he was blind, he had decided to end his life. A friend brought him to our clinic and his sight was restored. A tragic suicide was avoided.
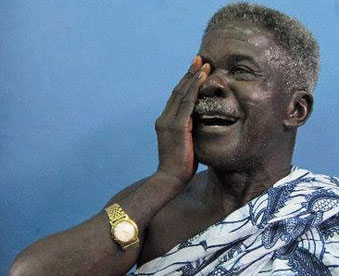
An African father and son were living a nomadic life begging for their daily needs. Their family had no resources to provide for them. The father’s sight was restored in one of our projects. “I am going back to farming to provide for my family. If Jesus loves me enough to send you here to help, then I have no problems with Jesus!” An entire family is saved from despair and hunger.
For more stories and impact CLICK HERE!
How it happens?
We are striving to have 200 Mentors on Missions, annually, by 2024 . Our work is divided into three areas: Missions, Training, and Networking.
MISSIONS
Our goal is to have “200 Mentors on Missions, annually, by 2024,” as we continue to administrate and support short-term cataract missions around the world.
TRAINING
We believe that quality Administrators, Medical Technicians, Physicians, and Spiritual leaders are needed to run a successful eye mission. Thus, we want to up our AMPS in training. We currently have 16 MSICS training camps a year for board certified ophthalmologists. We are in the process of developing a program to better equip the other areas.
NETWORKING
We believe that we are better when working together. This helps us minimize future mistakes and avoid duplication. We network with individuals, industries, and mission agencies around four core areas: Christ-likeness, International Missions, Eye Care Work, and Mentoring.
For more details on our work, CLICK HERE
Our main office is in the Great Lakes Eye Care building located in St. Joseph, Michigan.
2848 Niles Road,
Saint Joseph, MI 49085
Our primary office is in the Great Lakes Eye Care medical building. Our admin. # rings our cell phones.
Medical Office 269-428-3300
Admin. 269-588-0864
This email address goes to several individuals. Based on your content, one of us will reply.
GIVE WHERE NEEDED MOST
We will strive to daily hear and adhere to God’s word as written in the Bible, revealed through the life of Jesus and inspired by the Holy Spirit. I will strive to make His way – my way, His truth – my truth, and His life – my life as I become the word “made flesh” in my generation.
If you are paying for MULTIPLE Individuals (More than one registration) follow these steps.
If you have further questions, please contact us at [email protected]
We will strive to be a life-long learner, maintaining a teachable spirit in every situation and with every individual. I will use what I learn and share it with others, always striving to speak words that are meaningful, memorable, helpful, and repeatable. I will encourage everyone I teach to use what they have learned to teach others on a continual basis.
We will strive to give to, go on, or advocate for Global Eye Care Missions annually
We will strive to discipline ourselves to learn and improve our eye care skills like …
… in order to minimize the weights and distractions that seek to trip me and derail us and give full effort to accomplishing the goal of becoming the best eye care professional we can become.
MISSIONAL EYECARE AREAS OF LEADERSHIP
(M.A.P. S)
The NAME links below will take you to a webpage where you can download that specific E-pub reader.